Anesthesia Syringe Organization Hardware for Patient Safety
Team: BME Design Team: OR Smart
- Program: Biomedical Engineering
- Course:
Project Description:
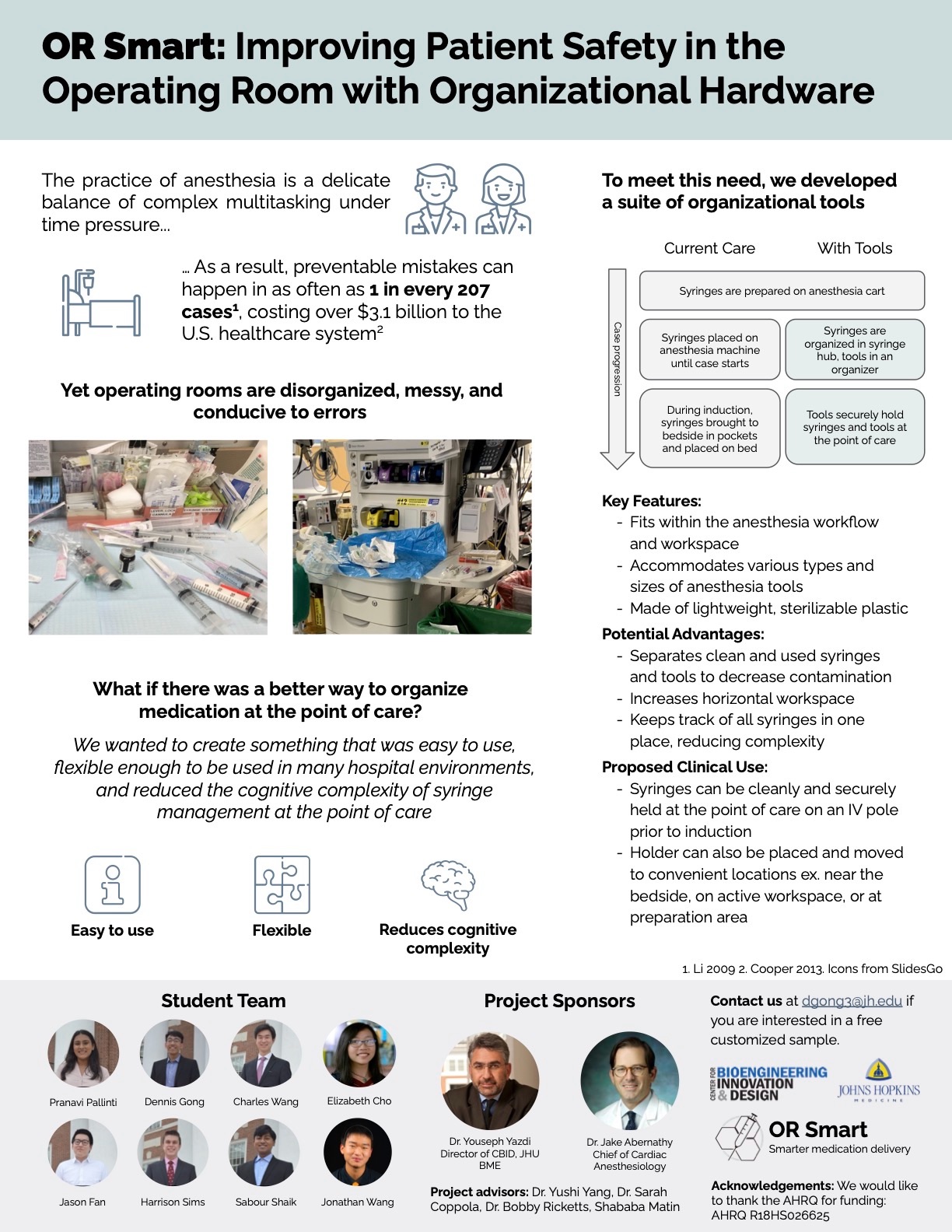
85-90% of anesthesia providers have committed at least one drug error or near miss in their careers. These errors are preventable; but still, complications for patients including death cost the U.S. healthcare system more than $1 billion annually. Specifically, syringe swaps in the operating room (OR), when the wrong syringe is inadvertently administered at the point of care, account for up to 44% of errors, affecting 24,000 patients annually in the U.S.. Syringe swap errors are considered the underlying cause of roughly 34 deaths annually, and are a contributing factor to another 281 deaths per year. In complex environments, like the OR anesthesia workspace, there are a multitude of reasons why syringe swaps can occur, the most common of which include failures to read or misreadings of vials and labels, lack of communication, inattention predisposed by production pressure, inaccurate labeling, distractions, and unfamiliar workplace equipment. The need for risk neutralizing ways to accurately identify and organize medications in the anesthesia workspace is acknowledged and studied, but no solutions with a strong evidence base have been implemented into clinical practice due in part to poor user experience. Our team is developing a tool to help anesthesia providers decrease cognitive burden, simplify the medication delivery system and more easily identify and administer medication in their chaotic operating room environment. Our key insight is that a solution that simplifies the provider experience will in turn reduce syringe swaps and other, similar medication errors. A flexible, adaptable, workflow simplifying solution has the potential to be introduced into every anesthesia requiring OR, more than 6,100 hospitals in the U.S. alone.
Project Photo: